The health system of Nigeria in 2015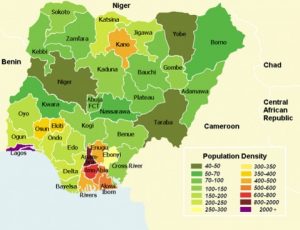
Nigeria has a population of approximately 200 million people, living in 36 states.
It is a country with a federal state structure where each state has substantial independence.
There are 774 LGA’s and about 32,000 health facilities. The country is vast and regions vary in density of population, level of urbanization and cul-tural traditions. Most of Nigeria’s health indicators are low as compared to GDP.
The challenge
The main health programs, being HIV, TB, Malaria, Vaccines and Reproductive Health, have been centrally managed, with a big input of donor funding, at the Ministry of Health in the federal capital Abuja. Supply of essential medicines to public hospitals is organized through the state Central Medical Stores operating a re-volving drug fund which procures and sells pharmaceuticals to public health facilities. This centralized man-agement of the health supply chain created little ownership at state level and below, thus creating a big chal-lenge for both management of products and obtaining good data.
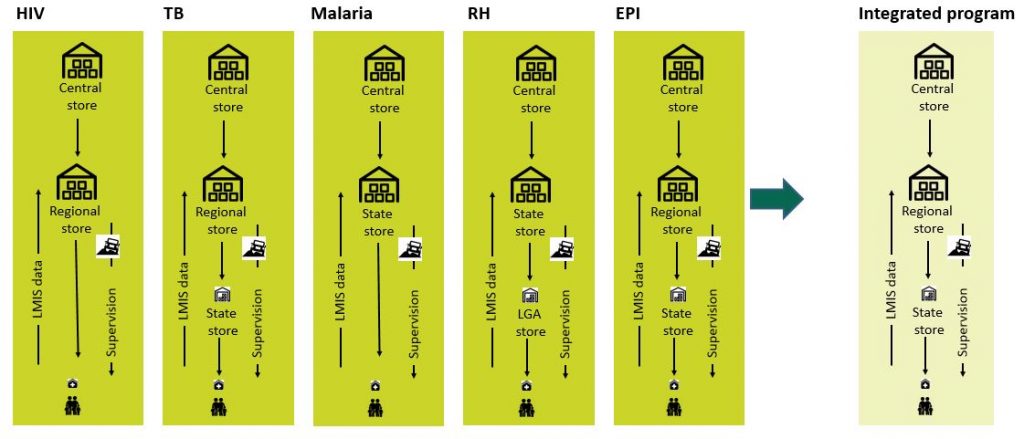
Each health program was in principle operated separately via allocated individual coordinators in each state and individual coordinators at LGA level. Each of the programs was supported by individual contractors working for the government of Nigeria and co-funded by donors such as USAID, GAVI, the Global Fund and UNFPA. These contractors developed separate data collection and separate product distribution mechanisms to facilitate supply to health facilities. The whole system was very much vertically organized and without co-ordination especially at the state level.
The purpose of the project
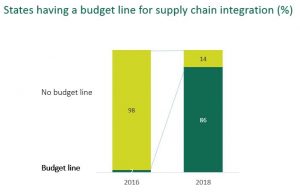
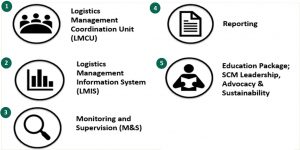
The Global Fund supported Nigeria Supply Chain Integration Project (NSCIP) of 2015 was aimed at enhancing (cost)-efficiency and effectiveness by integrating systems and coordinating actions. The project addressed both the combined collection of data across all health programs from the health facilities and the creation of coordination of warehousing and transportation at LGA, state and federal levels.
The creation of an integrated LMIS
Another part of the project was the creation of an aligned digital LMIS. This involved at first lengthy discus-sions with all the vertical programs centrally. We had to compare their existing paper based LMIS systems and to agree with them on where they could compromise and rationalize them, so we could create common forms and a common digital LMIS for all health programs.
Secondly we went on to set up a temporary solution in spreadsheets to finally integrate the LMIS solution in-to the Navision LMIS for the Vaccine program. This solution is running today.
The implementation
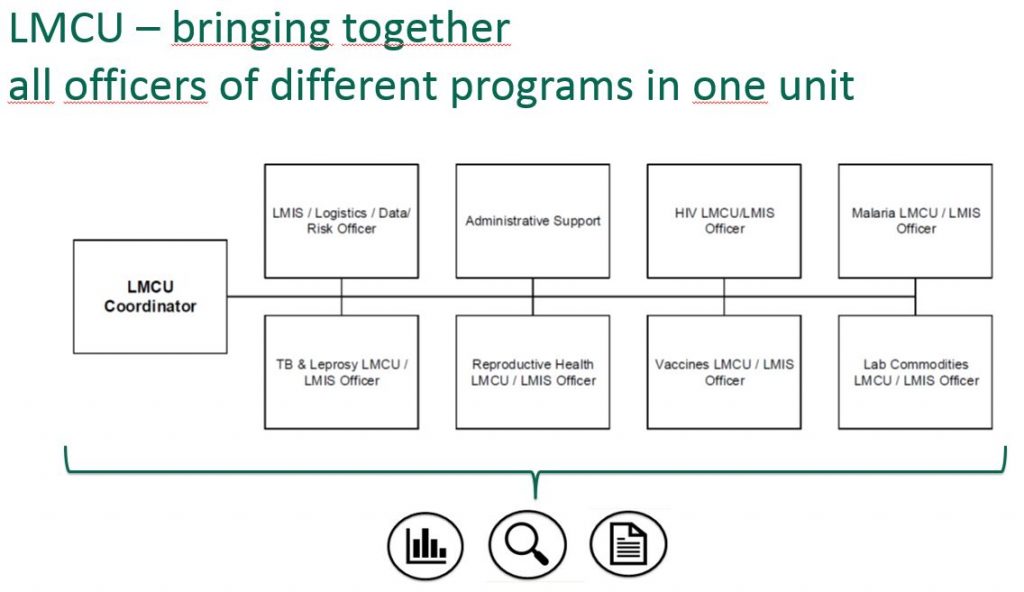
The full roll out took place through hiring change agents and placing them at each newly created LMCU. We used these change agents to train the staff of the LMCU and to assist in the roll out of the LMIS solution.
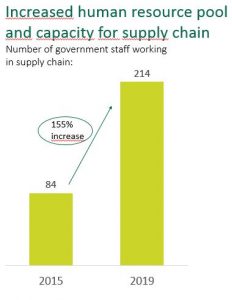
Three years later, LMCUs have been established as an institution and NSCIP is operating a national LMIS at a federal level for gathering data from HIV, Malaria, TB, and Reproductive health programs, whilst also working on adding more programs to the list. There is a lot more work to be done, but within the LMCUs, there are methods and Standard Operating Procedures in place. Also the key tool, the LMIS is operated as the tool to manage product flows.